
support@pattrac.info
This lesson describes how to create a new Encounter for a patient. An Encounter is each physical contact, or attempted contact with a patient.
Create a new Encounter
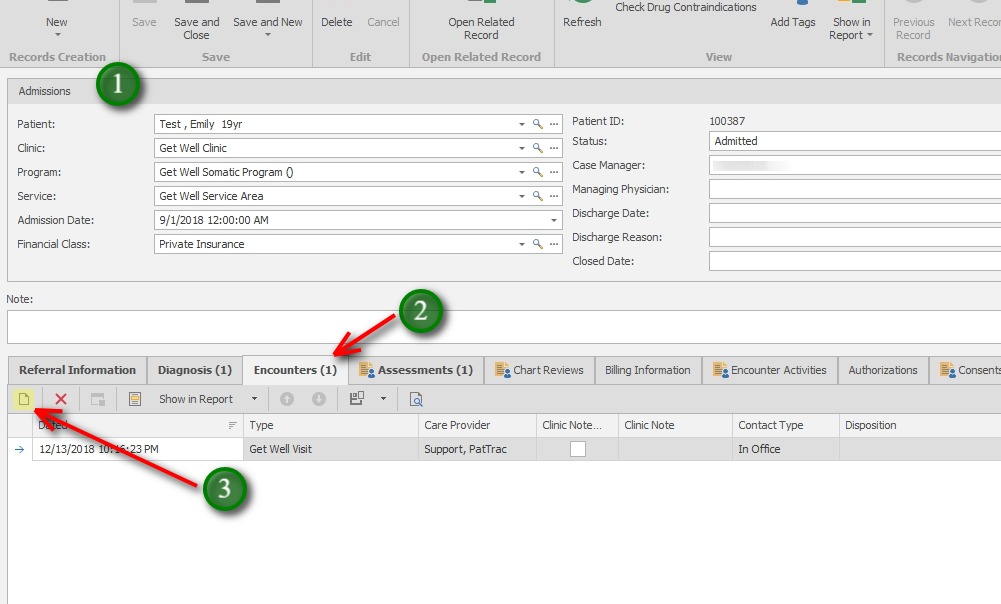
1. Open the Admission record for the Patient.
2. Click on the Encounters tab.
3. Click the “New” icon to add a new Encounter Record.
** Encounters are always attached to an Admission. An Admission record must exist before adding Encounters.
Complete the Encounter
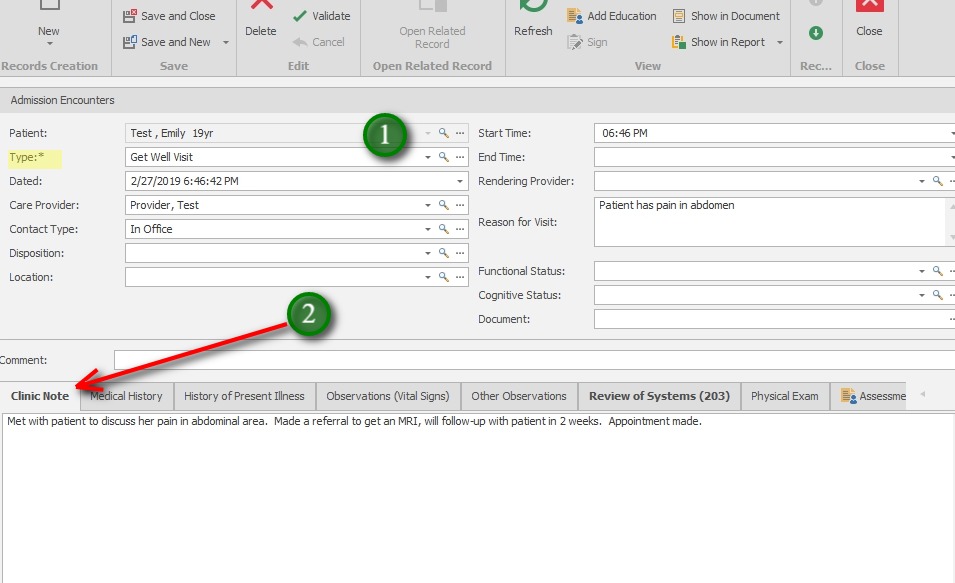
1. Encounter Information
Patient – this will auto-populate and is not editable.
Type – Select this REQUIRED field to choose the Encounter type.
**The Encounter Type will determine the tabs available at the bottom of the screen.
Dated – This will auto-populate with the current date/time of record creation.
Care Provider – Select the Care Provider for the Encounter.
Contact Type – optional field to define the Type of Contact with the client.
Disposition – optional field to indicate the Disposition of encounter.
Location – optional field to indicate the Location of the Encounter.
Start Time – This will auto-populate with the current time of record creation.
End Time – Enter the End Time of the encounter if required by the program.
Rendering Provider – Select Rendering Provider when applicable. (*In some cases this is required for claims billing)
Reason for Visit – this field is available only when the Encounter Type includes this option.
Functional & Cognitive Status – these are optional fields for the Encounter, however they may be required if exchanging data to an HIE.
Document – Optional field to attach a single document to an Encounter.
2. Clinic Note – If applicable enter the Visit Note, or Clinic note from the Encounter here. This Note can be locked and signed.
***Default tabs for an Encounter are Clinic Note, Diagnosis and Activities. All other tabs are optional to display. (Clinic > Maintain > Encounter Options.)